*QUALIA MIND IS NOT INTENDED TO DIAGNOSE, TREAT, CURE OR PREVENT ANY DISEASE. While we are encouraged by the results of this study, it was based on a multimodal therapeutic approach. As such, it is not possible to isolate the contribution, if any, of each of the interventions to the overall results. Therefore, these study results should not be interpreted as an indication that Qualia Mind reduces cognitive decline.
The Importance of Lifestyle Factors for Cognitive Health
As we age, cognitive health is determined by the combination of many different factors, some of them biological, but many, if not most, lifestyle-related. Diet, physical activity, stress, sleep, and socialization, for example, are among the main factors that can impact brain function. They may do so directly, but also as a consequence of influencing cardiovascular and metabolic health, gut health, and endocrine and immune function [1–4].
Therefore, attributing age-related cognitive decline to a specific cause is missing the whole picture. Likewise, targeting a single risk factor for cognitive decline is likely a less-than-ideal approach to adequately support cognitive health. A better approach is most likely one targeting multiple factors, both biological and lifestyle-related.
Several clinical trials and observational studies have supported this view by showing better outcomes in promoting cognitive health when multiple variables were addressed simultaneously. And even better than addressing multiple variables in a one-size-fits-all approach may be to tailor interventions to an individual’s specific history, lifestyle patterns, and risk factors—an individualized approach [5–12].
A recent study, led by Dr. Heather Sandison, ND, has added to the evidence that an individualized, multimodal, integrative care approach may promote healthier cognitive function. The study assessed the effects on cognitive health of a comprehensive intervention plan that included physical activity and dietary changes, nutritional support, and interventions aimed at supporting sleep, gastrointestinal, endocrine, and immune health, minimizing environmental toxicant exposure, and supporting detox. Supplements were part of the foundational intervention plan that all participants received. We’re proud to share that among them was Qualia Mind.*
How the Individualized Intervention Plan Was Designed
Participants were individuals aged 46 to 86 years with objective cognitive impairment as defined by clinically validated cognitive tests. In order to design the individualized care plan, participants received a thorough clinical assessment at baseline that included taking a full case history and a complete review of medications, supplements, lifestyle, diet, and exercise. A complete laboratory evaluation was performed (of blood, urine, hair, and stool samples) and nutrient status, metabolic, endocrine, cardiovascular, and gastrointestinal health (digestion and absorption, gut microbiota health, gut immune function) were evaluated, as well as biomarkers of environmental toxicant exposure (heavy metals, chemical pollutants, and biotoxins) and immune challenges potentially associated with cognitive decline. Based on these clinical evaluations, an intervention plan to be carried out over six months in a home setting was developed and discussed with each participant.
The intervention team included a clinician and a certified health coach. Throughout the 6 months study period, participants received weekly phone calls from their health coaches to assess challenges with the intervention plan, answer questions related to the interventions, discuss and adjust interventions, provide support and encouragement, and help participants maintain or improve adherence to the intervention plan.
Clinical visits then took place one, three, and six months after the beginning of the intervention. In these visits, participants’ responses to the intervention were evaluated, changes were tracked, laboratory results were reviewed, and the individualized intervention plan was discussed and adapted if needed.
Individualized Intervention Plan to Support Cognitive Health
The comprehensive intervention plan included a set of common foundational interventions along with individualized interventions based on each person’s biometric status and physical and logistical capacity.
As part of the foundational intervention, all participants received nutritional support, including a nootropic blend—Qualia Mind*—along with additional omega-3s, vitamin D, and probiotic support. All participants were initially recommended the same amounts of these supplements, but servings were later adjusted in response to lab results and individual responses and needs including tolerance, pill fatigue, and nutrient levels on testing.
To optimize metabolism, a ketogenic diet was encouraged, as well as a fasting period of a minimum of 12 hours each night, including three hours between the participant’s last meal and sleep. Consumption of organic produce, wild-caught low-mercury fatty fish high in omega-3s, organic, pastured eggs and poultry, organic dairy, and 100% grass-fed meats were encouraged. Participants were asked to eliminate alcohol, processed foods, and grains during the trial.
When indicated, improvement in digestion and nutrient assimilation was encouraged through the use of digestive enzymes, probiotics, gut healing nutrients (e.g., aloe, deglycyrrhizinated licorice, glutamine), gut immune support (colostrum, vitamin A, vitamin D, probiotics), pharmaceutical and/or herbal antimicrobials (e.g., nitazoxanide, oregano oil, etc.), as indicated by physiological signs and laboratory analysis.
Exercise recommendations were given based on participants’ characteristics and activity levels at baseline. Participants were encouraged to increase movement, get regular strength training and aerobic exercise, and adopt novel exercise routines. So instead of repeating exercises the participants were familiar with, the goal was to switch it up and find new activities. This is important because novelty is processed differently by the brain and is more stimulating than familiar stimuli, which supports brain plasticity.
Participants were also encouraged to increase social interaction and to engage in mindfulness practices of their choice such as meditation, gratitude practice, or prayer, for example. Sleep duration and quality were tracked and sleep hygiene was supported. When necessary, participants were referred to sleep medicine for further evaluation and intervention. Supplements to support sleep (e.g., melatonin, theanine, magnesium threonate, inositol, progesterone) were provided based on individual needs and responses.
Strategies to mitigate environmental exposures to toxicants were devised and support for hepatic detoxification was provided in the form of supplements (e.g., herbs, nutrients, glutathione), binding agents (e.g., cholestyramine, chlorella, charcoal, zeolite, clay), and chelating agents (e.g., EDTA, thiol-functionalized silica), along with sauna and lymphatic mobilization.
Immunity was supported by addressing immune challenges, adjusting diet and exercise, and with additional dietary supplementation (e.g., curcumin, glutathione, B vitamins, vitamin C, alpha-lipoic acid). Endocrine health was supported with bio-identical hormone replacement and/or herbal hormonal support when clinically appropriate.
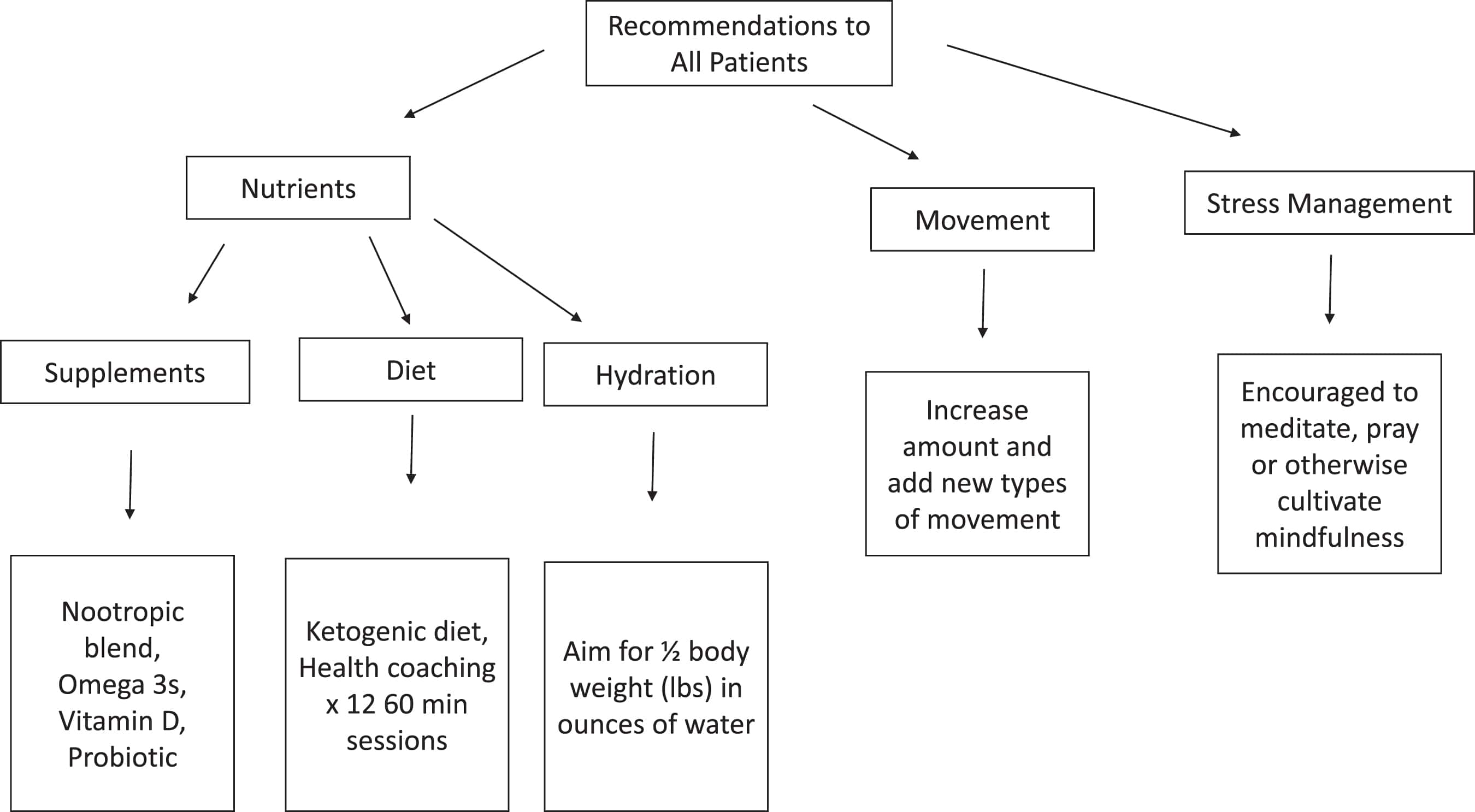
Figure 1 - Multimodal baseline strategies and intervention plans for optimizing cognitive health, prior to testing and individualized treatment. The nootropic blend mentioned in the figure is Qualia Mind*. Source: Sandison H, et al. J Alzheimers Dis. 2023; 94(3):993-1004. doi: 10.3233/JAD-230004. License: CC BY 4.0.
How the Individualized Intervention Plan Influenced Cognition
To evaluate the effect of the interventions, cognitive function was assessed throughout the study period using validated cognitive tests. Two tests were used: The Montreal Cognitive Assessment (MoCA), a test used clinically to assess and screen cognitive status, and The Cambridge Brain Sciences (CBS) test, a battery of 12 individual assessments designed to measure function in four cognitive domains—memory, reasoning, verbal ability, and concentration.
At the end of the six months, measures of cognition demonstrated that the individualized intervention plan promoted healthier cognitive performance. CBS neurocognitive tests showed a significant enhancement of memory (+10.6%) along with slight enhancements in concentration (+7.1%), reasoning (+4.7%), and verbal ability (+4.8%). Although only the memory domain met the statistical criteria to be deemed significant, all four domains revealed better mental performance after six months of intervention.
When the four domains were combined to analyze changes in overall cognition, a significant enhancement of 5.2% was determined. Overall cognition in the study population at baseline was at the 24th percentile compared to age and gender-matched scores from a large data set of healthy individuals (over 75,000 healthy individuals, with the 50th percentile being defined by their average cognitive scores). The 5.2% change moved participants to the 29th percentile, which may be regarded as a meaningful gain toward normal cognitive function. Likewise, memory in the study population at baseline was at the 25th percentile (demonstrating objective decline compared to the database of healthy individuals) and the ~11% enhancement moved participants to the 35th percentile.
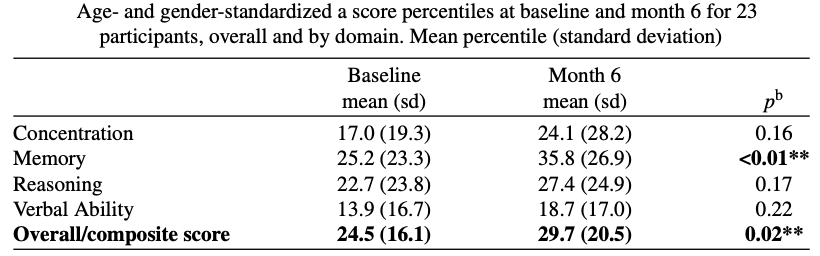
Figure 2 - Score percentiles at baseline and month six. Source: Sandison H, et al. J Alzheimers Dis. 2023; 94(3):993-1004. doi: 10.3233/JAD-230004. License: CC BY 4.0.
Another noteworthy finding was that more than 50% of the 23 participants showed enhancements in each of the four domains of cognitive testing: concentration was enhanced or stable in 55% of participants; memory in 82%; reasoning in 64%; and verbal ability in 68%. The overall score showed enhancements or maintenance in 74% (n = 17) of participants. Cognitive status scores (i.e. MoCA scores) at six months compared to baseline were also found to be enhanced or stable in 74% (n = 17) of participants.
Only 26% of participants showed further cognitive decline that would be expected with the natural course of their condition. MoCA scores in individuals with measurable cognitive impairment receiving standard of care are expected to steadily decline, on average at a rate of 2.39 points or greater per year [13].
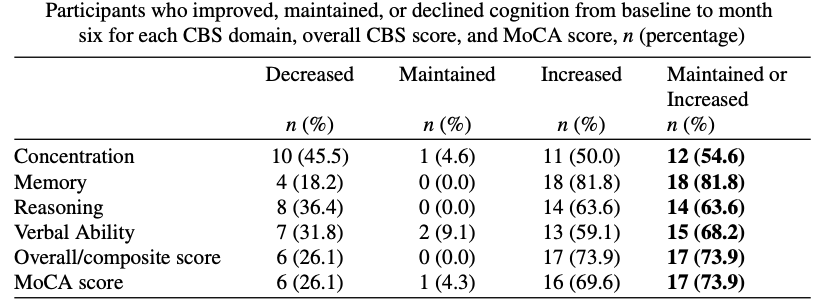
Figure 3 - Number and percentage of participants who improved, maintained, or declined cognition from baseline to month six. Source: Sandison H, et al. J Alzheimers Dis. 2023; 94(3):993-1004. doi: 10.3233/JAD-230004. License: CC BY 4.0.
A change of ±1.73 points in the MoCA score is regarded as clinically meaningful [14]. After six months of individualized intervention, study participants showed, on average, an enhancement of over 2 points, indicating a clinically meaningful inflection in progression. MoCA scores range from 0 to 30, with scores equal to or above 26 indicating normal cognition and scores equal to or below 25 indicating impaired cognition [15]. At the beginning of the study, all participants had MoCA scores below 23, indicating objective cognitive impairment (it was an inclusion criterion for the study). But by the end of the intervention, six participants had scores equal to or above 26, indicating a reversal of cognitive impairment, the best outcome that could be expected.
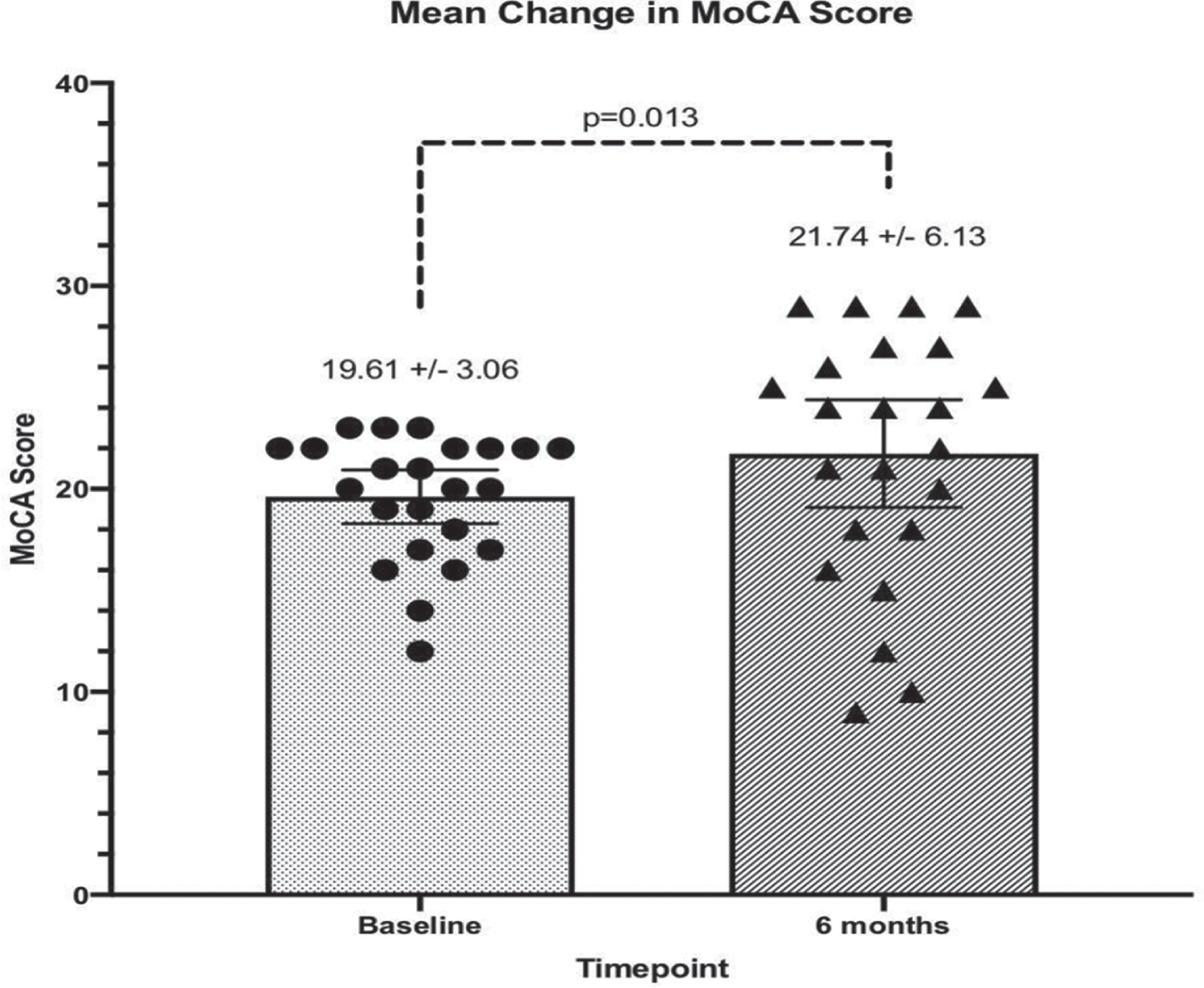
Figure 4 - MoCA test scores of at baseline and after six months of intervention. Source: Sandison H, et al. J Alzheimers Dis. 2023; 94(3):993-1004. doi: 10.3233/JAD-230004. License: CC BY 4.0.
It’s important to note that this was a small trial with no placebo control. Further research is needed in larger, controlled clinical trials that may evaluate more accurately the applicability of this approach to support the management of cognitive decline. Nevertheless, these results demonstrate meaningful changes to cognitive function that indicate that multimodal, individualized care plans are a feasible and potentially helpful strategy for the management of cognitive health with aging.
How Qualia Mind May Support Cognitive Heath*
Qualia Mind combines 27 ingredients that have been carefully selected to support mental energy, alertness, attention, concentration, focus, memory, mood, motivation, and overall cognitive performance.* It contains nootropic compounds, neuro-vitamins, amino acids, choline donors, and herbal adaptogens.
Qualia Mind supplies resources for the brain. It provides nutrients and precursors necessary for healthy cognitive function, along with ingredients that help the brain make good use of those nutrients.*
Qualia Mind was designed with the goal of supporting key neural pathways and processes. It contains nootropic compounds, neuro-vitamins, amino acids, choline donors, and herbal adaptogens. Each ingredient has stand-alone actions; they also have additive actions when combined, complementing each other in support of cognitive pathways or processes.*
We invite you to read Qualia Mind: The Building of a Nootropic Stack to better understand the thought processes behind the formulation of Qualia Mind. If you want to learn more about Neurohacker Collective’s formulating principles you may also read Qualia: The Complex Intelligence Behind Its Formulation and Neurohacker Dosing Principles.
*QUALIA MIND IS NOT INTENDED TO DIAGNOSE, TREAT, CURE OR PREVENT ANY DISEASE. While we are encouraged by the results of this study, it was based on a multimodal therapeutic approach. As such, it is not possible to isolate the contribution, if any, of each of the interventions to the overall results. Therefore, these study results should not be interpreted as an indication that Qualia Mind reduces cognitive decline.
Other References
[1]N. Kimura, Y. Aso, K. Yabuuchi, M. Ishibashi, D. Hori, Y. Sasaki, A. Nakamichi, S. Uesugi, H. Fujioka, S. Iwao, M. Jikumaru, T. Katayama, K. Sumi, A. Eguchi, S. Nonaka, M. Kakumu, E. Matsubara, Front. Neurol. 10 (2019) 401.
[2]S. Song, Y. Stern, Y. Gu, Ageing Res. Rev. 74 (2022) 101551.
[3]J.S. Randolph, J.J. Randolph, in: J.J. Randolph (Ed.), Positive Neuropsychology: Evidence-Based Perspectives on Promoting Cognitive Health, Springer New York, New York, NY, 2013, pp. 25–55.
[4]M. Yuan, J. Chen, Y. Han, X. Wei, Z. Ye, L. Zhang, Y.A. Hong, Y. Fang, Int. Psychogeriatr. 30 (2018) 1465–1476.
[5]D.E. Bredesen, Aging 6 (2014) 707–717.
[6]D.E. Bredesen, E.C. Amos, J. Canick, M. Ackerley, C. Raji, M. Fiala, J. Ahdidan, Aging 8 (2016) 1250–1258.
[7]D.E. Bredesen, K. Sharlin, D. Jenkins, M. Okuno, W. Youngberg, S.H. Cohen, A. Stefani, R.L. Brown, S. Conger, C. Tanio, A. Hathaway, M. Kogan, D. Hagedorn, E. Amos, A. Amos, N. Bergman, C. Diamond, J. Lawrence, I.N. Rusk, P. Henry, M. Braud, J. Alzheimers Dis. Parkinsonism 08 (2018).
[8]R.V. Rao, S. Kumar, J. Gregory, C. Coward, S. Okada, W. Lipa, L. Kelly, D.E. Bredesen, Biomedicines 9 (2021).
[9]N. Schneider, C. Yvon, J. Nutr. Health Aging 17 (2013) 252–257.
[10]T. Ngandu, J. Lehtisalo, A. Solomon, E. Levälahti, S. Ahtiluoto, R. Antikainen, L. Bäckman, T. Hänninen, A. Jula, T. Laatikainen, J. Lindström, F. Mangialasche, T. Paajanen, S. Pajala, M. Peltonen, R. Rauramaa, A. Stigsdotter-Neely, T. Strandberg, J. Tuomilehto, H. Soininen, M. Kivipelto, Lancet 385 (2015) 2255–2263.
[11]G. Schechter, G.K. Azad, R. Rao, A. McKeany, M. Matulaitis, D.M. Kalos, B.K. Kennedy, J Alzheimers Dis Rep 4 (2020) 223–230.
[12]M. Fotuhi, B. Lubinski, M. Trullinger, N. Hausterman, T. Riloff, M. Hadadi, C.A. Raji, J Prev Alzheimers Dis 3 (2016) 133–137.
[13]M. Miyakawa-Liu, A.K. Feehan, S. Pai, J. Garcia-Diaz, Ochsner J. 22 (2022) 129–133.
[14]K. Krishnan, H. Rossetti, L.S. Hynan, K. Carter, J. Falkowski, L. Lacritz, C.M. Cullum, M. Weiner, Assessment 24 (2017) 772–777.
[15]Z.S. Nasreddine, N.A. Phillips, V. Bédirian, S. Charbonneau, V. Whitehead, I. Collin, J.L. Cummings, H. Chertkow, J. Am. Geriatr. Soc. 53 (2005) 695–699.
No Comments Yet
Sign in or Register to Comment